Mastering the NEET PG demands a strategic approach to preparation, with an emphasis on high-yield topics proving to be a successful tactic. This blog zeroes in on exactly that – a curated list of high-yield questions in Anatomy that are highly likely to appear on the NEET PG.
1.Arrange the following events of pre-embryonic development in order, from the earlier stage to the later stage.
- Cavitation
- Compaction
- Implantation
- Cleavage
a: 2- 4- 1- 3
b: 3 -1- 2 – 4
c: 4 – 2- 3- 1
d: 4 – 2- 1- 3
Solution: Correct answer is ‘d’ i.e., 4 – 2 – 1 – 3
The correct order of the listed events of the pre-embryonic period is cleavage – compaction – cavitation – implantation.
Events of the pre-embryonic phase of development:
- Fertilization
- Cleavage – Formation of blastomeres; the cells are loosely arranged until the 8 cell stage.
- Compaction – After 3 cleavages, the blastomeres are held together by tight junctions.
- Differentiation – The compacted 8 cell stage divides to form a 16 cell morula.
- Cavitation – Formation of the blastocyst with inner cell and outer cell mass.
- Hatching of the blastocyst – Release of the blastocyst from the zona pellucida.
- Implantation – Attachment of developing embryo to the uterine endometrium.
- Cell mass differentiation – Differentiation of the embryoblast (inner cell mass) into columnar epiblast cells and cuboidal hypoblast cells.
- Bilaminar disc formation – Formation of the bilaminar disc suspended by the connecting stalk. It has two layers (epiblast and hypoblast) and two cavities (amniotic and yolk sac).
2: A 45 year old man had a CT scan to evaluate a lower respiratory tract infection. Incidentally, he was found to have a left-sided superior vena cava draining into the coronary sinus. The patient reported no cardiac symptoms. Failure of regression of which of the following structures during embryonic development leads to the given anatomical variation?
a: Left anterior cardinal vein
b: Right anterior cardinal vein
c: Left common cardinal vein
d: Right posterior cardinal vein
Solution: Correct answer is ‘a’ i.e., Left anterior cardinal vein
Persistent left-sided superior vena cava occurs due to failure of regression of the left anterior cardinal vein. It may drain either into the coronary sinus or the left atrium.
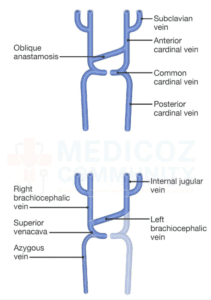
The formation of the vena cava system begins with the formation of anastomoses between the right and left venous channels. Formation of the major veins takes place as follows:
- The proximal part of the right anterior cardinal vein along with the right common cardinal vein form the superior vena cava
- The distal part of the right anterior cardinal vein between the junction with the subclavian vein and the junction with the transverse anastomosis becomes the right brachiocephalic vein
- The distal part of the left anterior cardinal vein and the transverse anastomosis becomes the left brachiocephalic vein
- The most cranial part of both the anterior cardinal veins above its junction with subclavian vein become the internal jugular vein
3: A 5 day old infant was admitted to the NICU as she was suffering from severe dyspnea and cyanosis. Chest X-ray revealed hypoplastic left lung and herniation of the intestines into the left thoracic cavity. Abnormality in which of the following structures during the embryonic development will most commonly lead to the given condition?
a: Mesentery of the esophagus
b: Pleuropericardinal folds
c: Body wall
d: Pleuroperitoneal folds
Solution: Correct answer is ‘d’ i.e., Pleuroperitoneal folds
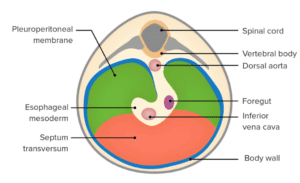
The given clinical scenario is suggestive of a congenital diaphragmatic hernia. It most commonly occurs due to failure of fusion of pleuroperitoneal folds during the development of the diaphragm.
The diaphragm develops from 4 mesodermal sources as follows;
- Septum transversum becomes the anterior and medial part of the diaphragm including the central tendon
- Pleuroperitoneal membranes (paired structures) become the dorsolateral parts of the diaphragm
- Mesoderm of body wall from somites of cervical segments three to five (C3-5) contribute to the peripheral muscular part
- Mesentery of the esophagus forms the crura of the diaphragm
- Congenital diaphragmatic hernia results due to failure of various structures forming diaphragm to fuse. It occurs in 1/2000 births. The defect allows abdominal viscera to enter the pleural cavity. It is most frequently caused by the failure of one or both of the pleuroperitoneal membranes to fuse. Posterolateral defects (Bochdalek’s hernia) are the most common (85 – 90%).
Development of Diaphragm
4: A 48 year old woman presented with thyroid swelling. After evaluation, it was diagnosed as medullary thyroid cancer. Calcitonin produced from parafollicular C cells was used as a prognostic marker. These cells are derived from which structure?
a: 3rd pharyngeal cleft
b: 3rd pharyngeal pouch
c: 4th pharyngeal cleft
d:Ultimobranchial body
Solution: Correct answer is ‘d’ i.e., Ultimobranchial body
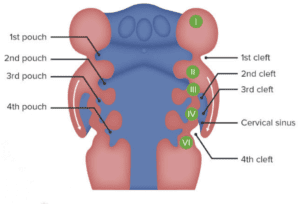
Calcitonin produced by parafollicular C-cells of the thyroid which is derived from the ultimobranchial body (4th pharyngeal pouch derivative).
The 4th pharyngeal pouch develops a small diverticulum medial to the main pouch called the ultimobranchial body. The ultimobranchial body is later incorporated into the thyroid gland and its cells give rise to the parafollicular or C-cells of the thyroid gland. These cells secrete a hormone called calcitonin that is involved in the regulation of the calcium level in the blood.
Clinical consideration: Both chromaffin cells of the adrenal medulla and parafollicular cells (C-cells) of the thyroid originate from the neural crest cells. A common, germ-line mutation in neural crest cells can cause tumors in both the adrenal medulla and the thyroid, as seen in MEN types 2A and 2B.
Pharyngeal Pouch Derivatives
5: The site in the pharyngeal arch where the ectodermal cleft meets the endodermal pouch is known as:
a: Pharyngeal cleft
b: Pharyngeal pouch
c: Pharyngeal membrane
d: Cervical sinus
Solution: Correct answer is ‘c’ i.e., Pharyngeal membrane
The pharyngeal membrane is the location where the ectoderm of the pharyngeal cleft meets the endoderm of the pharyngeal pouch.
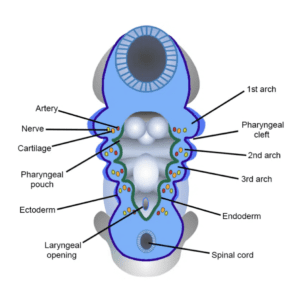
In the interval between any two adjoining pharyngeal arches, the endoderm extends outward in the form of a pouch (pharyngeal pouch) to meet the ectoderm, which dips into this interval as a pharyngeal cleft. The membrane formed where the pharyngeal cleft comes in contact with the pouch is called the pharyngeal membrane.
Initially, there are four pharyngeal membranes between the five arches. Only the first pharyngeal membrane develops and contributes to the formation of the tympanic membrane. The 2nd, 3rd, and 4th pharyngeal membranes do not develop further into any structure. They get obliterated when the mesoderm from the 2nd arch overgrows and fills the succeeding cleft.
Pharyngeal Apparatus
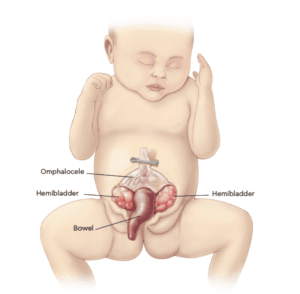
6: You note the given finding in a baby admitted to the pediatric ward. Which of the following defects in the intrauterine life is the cause of this condition?

a: Failure of the intestinal loops to return from umbilicus
b: Defective closure of body wall in the abdominal region
c: Defective closure of body wall in the pelvic region
d: Defective closure of the vitellointestinal duct
Solution: Correct answer is ‘c’ i.e., Defective closure of body wall in the pelvic region
The condition shown in the image is cloacal exstrophy, which is caused by the failure of the body wall to close in the pelvic region.
The given image shows the classic feature of cloacal exstrophy, which includes an exstrophic central bowel area flanked by two hemibladders;
- Bladder exstrophy: The bladder is seen turned inside out (exstrophy means turned inside out) and visible as 2 hemibladders on either side.
- Bowel exstrophy: The central defect is the prolapsed intestinal loop that appears as the elephant trunk deformity. The central bowel field usually contains an ileocecal segment that has prolapsed.
- In addition, omphalocele can be noted in the umbilical region in this image.
Cloacal Exstrophy
Exstrophy of the bladder or cloaca occurs due to abnormal closure of the body wall in the pelvic region:
- Exstrophy of the bladder: The bladder mucosa is exposed to the surface. In male infants, epispadias is seen additionally.
- Exstrophy of the cloaca: The closure of the ventral body wall is more severely affected than in bladder exstrophy. There is the involvement of the bladder and rectum, both of which are derived from the cloaca. In addition, there is defective development of the urorectal septum leading to anal canal malformations and imperforate anus. As the genital swellings are widely separated, external genitalia will be defective.
Cloacal exstrophy can present as part of OEIS syndrome, in which multiple anomalies are seen, where O stands for Omphalocele, E for Exstrophy of bladder or cloaca, I for Imperforate anus, and S for Skeletal anomalies.
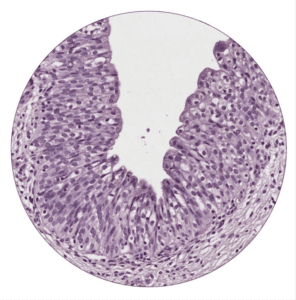
7: The type of epithelium as shown in the image below is present in ________
a: Duodenum
b: Common bile duct
c: Skin
d: Urinary bladder
Solution: Correct answer is ‘d’ i.e., Urinary bladder
The type of epithelium shown in the image is the transitional epithelium and it is present in the urinary bladder.
Transitional epithelium is a specialized epithelium lining most of the urinary tract, hence it is also called the urothelium. The deepest layer consists of columnar or cuboidal cells, and the middle layer consists of polyhedral or pear – shaped cells. The surface layer consists of large, polypoid, dome shaped, or umbrella –shaped cells. As the epithelium gets stretched to accommodate urine, the surface cells become flattened. The cells are called transitional due to this apparent change (transition) from stratified cuboidal epithelium in a relaxed state to stratified squamous epithelium when it is stretched.
They are present in:
- Collecting ducts
- Renal pelvis and calyces
- Ureter
- Urinary bladder
- Pre-prostatic and prostatic parts of urethra
8: A 43 year old man presented to the clinic with a history of anemia, non-bloody diarrhoea and poor appetite. A diagnosis of celiac disease is suspected and a duodenal biopsy is taken for histopathological examination. Which of the following cells are not likely to be seen on microscopic examination of the section?
a: Stem cells
b: Goblet cells
c: Paneth cells
d: Neck cells
Solution: Correct answer is ‘d’ i.e., Neck cells
Neck cells are not likely to be seen on microscopy as they are not present in the small intestine. The neck cells are the mucous secreting cells that are present in the upper end (or ‘neck’) of the main gastric glands of the stomach.
Option A: Stem cells are the undifferentiated cells present in the wall of the intestinal crypts.
Option B: Goblet cells are mucous secreting cells. Each goblet cell has an expanded upper part that is distended with mucin granules. The nucleus is flattened and is situated near the base of the cell.
Option C: Paneth cells (zymogen cells) are found only in the deeper parts of intestinal crypts. They contain prominent eosinophilic secretory granules.
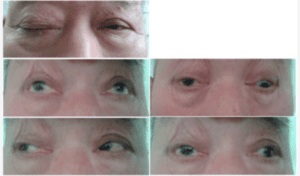
9: Which of the following statements regarding the nerve involved in the palsy shown below is false?
a: It divides into upper and lower divisions in the anterior part of the cavernous sinus.
b: Its divisions enter the orbit through the middle part of the superior orbital fissure.
c: It lies between the posterior cerebral and superior cerebellar arteries in the interpeduncular fossa.
d: The nerve to inferior rectus carries parasympathetic fibers to the ciliary ganglion
Solution: Correct answer is ‘d’ i.e., The nerve to inferior rectus carries parasympathetic fibers to the ciliary ganglion
The image shows oculomotor nerve palsy. The nerve to inferior oblique carries parasympathetic fibers to the ciliary ganglion, not the nerve to inferior rectus.
Course of the oculomotor nerve:
- The nerve lies on the anterior surface of the midbrain in between the posterior cerebral artery and the superior cerebellar artery in the interpeduncular fossa.
- It then passes to the middle cranial fossa along the lateral dural wall of the cavernous sinus and divides into superior and inferior in its anterior part.
- It enters the superior orbital fissure through the common tendinous ring.
10:
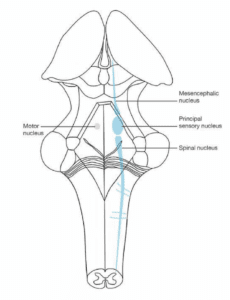
Which of the following sensations is not perceived by the spinal nucleus of the trigeminal nerve?
a:Temperature
b:Pain
c: Touch
d: Proprioception
Solution: Correct answer is ‘d’ i.e., Proprioception
Proprioception is perceived by the mesencephalic nucleus of the trigeminal nerve, not the spinal nucleus.
The trigeminal nerve consists of 4 nuclei: 3 sensory (Mesencephalic, spinal, and principal sensory nucleus) and 1 motor.
Nuclei of Trigeminal Nerve
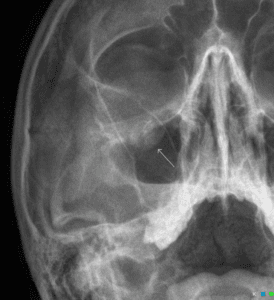
11:A 25 year old man presents to the ER after receiving a punch to the right side of his face. His X-ray is shown below. Which of the following bones maximally contributes to the region fractured?
a: Maxilla
b:Sphenoid bone
c: Palatine bone
d: Zygomatic bone
Solution: Correct answer is ‘a’ i.e., Maxilla
The X-ray shows a fracture of the floor of the orbit. The maximum contribution to the floor of the orbit is by the maxilla.
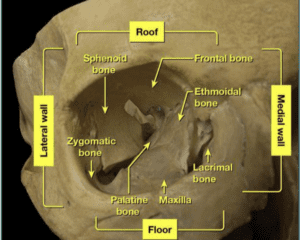
Boundaries of the bony orbit:
- Roof
- Orbital plate of frontal bone
- Sphenoid bone (small part)
- Floor: Thin plate of bone that also forms the roof of the maxillary sinus
- Orbital plate of maxilla
- Zygomatic bone (anterolateral)
- Orbital process of palatine bone (posteromedial)
- Medial wall:
- Maxilla
- Lacrimal bone
- Ethmoid bone
- Sphenoid bone
- Lateral wall:
- Zygomatic bone (anterior)
- Greater wing of sphenoid (posterior)
- Sphenozygomatic suture.
Bone Forming the Orbit
The orbital floor can be fractured by trauma to the orbit as seen in falls, motor vehicle accidents, and assaults. The image given shows X-ray Water’s view with a ‘teardrop’ sign. The orbital contents leak out of the fractured orbital floor, giving it a teardrop-like appearance.
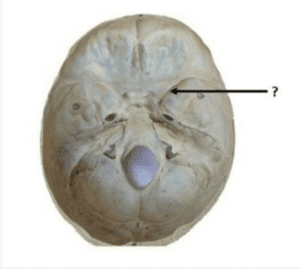
12: Identify the structure passing through the foramen marked.
a: Abducens nerve
b: Spinal accessory nerve
c: Ophthalmic artery
d: Middle meningeal artery
Solution: Correct answer is ‘a’ i.e., Abducens nerve
The marked foramen is the superior orbital fissure and the abducens nerve passes through it.
The abducens nerve is the 6th cranial nerve and arises from the brainstem at the pontomedullary junction. It runs through the Dorello’s canal which is present at the medial most end of the petrous ridge and then enters the cavernous sinus where it lies lateral to the internal carotid artery. It enters the orbit through the superior orbital fissure within the common tendinous ring and supplies the lateral rectus.
Other options:
Spinal accessory nerve passes through the foramen magnum along with the medulla oblongata and the vertebral arteries
Ophthalmic artery passes through the optic canal along with the optic nerve.
Middle meningeal artery and vein pass through the foramen spinosum along with the meningeal branch of mandibular nerve.
Structures passing through the Superior orbital fissure
Above the common tendinous ring: LFT (Superolateral compartment)
- Lacrimal nerve
- Frontal nerve
- Trochlear nerve
- Superior ophthalmic vein
Within the common tendinous ring: BAN (Intermedial compartment)
- Both divisions of oculomotor nerve
- Abducens nerve
- Nasociliary nerve
- Below the common tendinous ring (inferomedial compartment)
- Inferior ophthalmic vein
13: A 16 year old boy presented with instability of the shoulder joint following sports trauma. Injury to all of the following structures may cause this condition except:
a: Teres major
b: Supraspinatus
c: Tendon of long head of biceps
d: Coracoacromial ligament
Solution: Correct answer is ‘a’ i.e., Teres major
Teres major has no role in maintaining the stability of the shoulder joint.
The shoulder joint is a ball and socket joint. Since the head of the humerus is larger than the glenoid cavity, it is often prone to displacement. However, the stability of the shoulder joint is provided by the following:
- Rotator cuff: It is formed by blending of tendons of 4, muscles (SITS) –
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
- Tendon of the long head of biceps: It passes over the head of the humerus and prevents upward displacement.
- Coracoacromial ligament
Degeneration or tear of the above structures leads to instability of the shoulder joint.
The shoulder joint is least protected inferiorly. The capsule is loose and only one muscle crosses the joint inferiorly i.e., long head of triceps.
14: A 33 year old male was brought to the emergency department after being injured in mob violence. The patient had a penetrating injury in the right shoulder region by a sharp glass piece. On examination, there was drooping of the right shoulder associated with winging of the scapula. Which of the following nerves is likely to be injured?
a: Long thoracic nerve
b:Thoracodorsal nerve
c: Spinal accessory nerve
d: Dorsal scapular nerve
Solution: Correct answer is ‘c’ i.e., Spinal accessory nerve
Injury to the spinal accessory nerve can cause both drooping of the shoulder and winging of the scapula.
The trapezius is innervated by the spinal accessory nerve (CN XI). It causes:
- Retraction of scapula
- Shrugging of the shoulder
- Overhead abduction (along with serratus anterior)




Leave feedback about this
You must be logged in to post a comment.